This procedure allows the doctor to examine the nasal passages and sinuses closely. Using a small instrument called an endoscope, inserted gently through the nose, the doctor can look for signs of infection, nasal polyps, tumors, or structural abnormalities. It is especially helpful for people with chronic sinus problems or unexplained nasal blockage.
The procedure is usually done while you are awake. A numbing spray may be used in the nose to reduce discomfort. Patients can go back to normal activities right away. There is no effect on speech or breathing after this procedure. Occasionally, mild nosebleeds or irritation can occur, but these are rare. The procedure helps guide further treatment, such as surgery, medication, or allergy care.
Diagnostic esophagoscopy is a procedure used to look inside the esophagus, which carries food from the mouth to the stomach. It is used to diagnose the causes of swallowing difficulty, pain, or suspected tumors or strictures in the esophagus. The doctor uses a long, flexible tube with a light and camera to inspect the esophagus.
Depending on the patient's condition, the procedure may be done with mild sedation or general anesthesia. Sometimes, it can be done in the office setting. It is generally safe and does not affect speech. After the procedure, your throat might feel sore, and you may need to avoid eating or drinking for a short period. Any findings may require a biopsy, and depending on the results, follow-up may include dietary changes, medications, or additional treatments.
This procedure combines two techniques—dilation to widen narrowed airways and excision to remove abnormal tissue. It is often performed in patients with airway stenosis, tumors, or inflammatory lesions that are blocking normal airflow. This approach helps restore breathing and can reduce coughing, wheezing, or noisy breathing.
Diagnostic Bronchoscopy can sometimes be done in the office with local anesthesia.
Bronchoscopy is performed under general anesthesia. A bronchoscope is used to access the airway. A balloon or rigid dilator is inflated to widen the narrowed section, and surgical instruments or a laser may be used to remove excess tissue. Afterward, patients are monitored for breathing and airway swelling. Voice is usually unaffected unless the lesion is near the vocal cords. Multiple treatments may be necessary in chronic cases, and follow-up often includes imaging or repeat scoping to ensure long-term airway patency.
Transoral endoscopy is a procedure in which an endoscope is passed through the mouth to examine areas such as the throat, larynx, and upper esophagus. It is commonly used for patients with voice issues, swallowing difficulties, or suspected tumors. This approach provides a clear view and allows minor procedures, such as biopsies, to be done simultaneously.
Microflap surgery is a delicate procedure to remove benign growths on the vocal cords, such as cysts, polyps, or other cysts, while preserving the surrounding vocal tissue. During this surgery, the doctor creates a tiny flap in the surface of the vocal fold, gently lifts it, and removes the lesion beneath. This method minimizes scarring and preserves the patient's voice quality.
The procedure is performed under general anesthesia using a microscope and microsurgical tools. After surgery, patients are usually placed on strict voice rest for a few days, followed by a gradual return to speaking. Voice therapy is often recommended to optimize healing and prevent recurrence. Risks include scarring, temporary hoarseness, or, less commonly, changes to voice quality. Recovery is usually smooth, and the surgery often significantly improves vocal function.
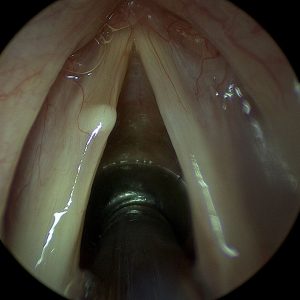
Before: Microflap Surgery for a Vocal Fold Cyst

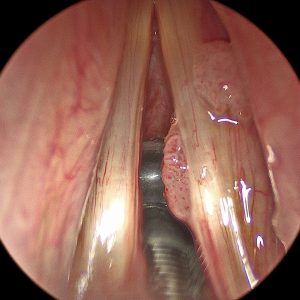
After: Microflap Surgery for a Vocal Fold Cyst
Microlaryngoscopy with excisional biopsy involves surgically removing a small piece of tissue from the vocal cords or larynx to be examined under a microscope. It is used when an unknown lesion or abnormality, such as a nodule, mass, or ulcer, is present and a precise diagnosis is needed.
This procedure is done under general anesthesia using specialized tools through the mouth. Through a microscope, the surgeon views the vocal cords and carefully removes the target tissue. Afterward, patients are typically advised to rest their voice and may feel mild throat discomfort. Results from the biopsy usually guide further treatment. The risk of complications is low, and speech is usually unaffected once healing is complete, though some patients may need follow-up procedures or therapy based on the biopsy results.
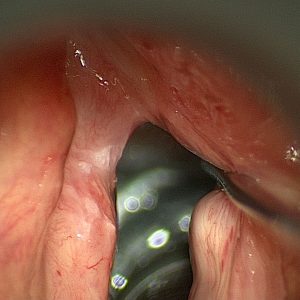
Before: Microlaryngoscopy removal of Leukoplakia
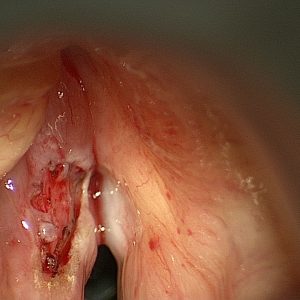
After: Microlaryngoscopy removal of Leukoplakia
This procedure involves using a CO2 laser to remove papillomas—wart-like growths caused by the human papillomavirus (HPV)—from the vocal folds. If they grow large or recur, papillomas can cause hoarseness, voice changes, and breathing issues. Laser excision allows for precise removal of these lesions while preserving surrounding healthy tissue.
Under general anesthesia, the surgeon uses a micro laryngoscope to access the vocal folds and a CO2 laser to vaporize or cut away the papillomas. This technique is less invasive and allows for quicker recovery with minimal bleeding. Patients are advised to rest their voice following surgery and may need repeated procedures if the papillomas return. Risks include temporary hoarseness, vocal cord scarring, or recurrence of the papillomas, which is common in some cases due to the viral nature of the disease.
Before: CO2 Laser Excision of Papilloma

After: CO2 Laser Excision of Papilloma
Laser cordectomy is a surgical procedure that uses a precise laser beam to remove cancerous tissue from the vocal cords. It is often performed in early-stage laryngeal cancer, where preserving voice and airway function is important. Depending on the amount of tissue that needs to be removed, the procedure is categorized into types I through VI.
Performed under general anesthesia, the surgeon uses a laser to excise the cancerous areas while minimizing damage to surrounding structures. The more extensive the resection (higher type number), the greater the impact on voice. Recovery includes a period of voice rest and follow-up visits to monitor healing. Some patients may notice a permanent change in voice quality, and voice therapy may be recommended. The procedure avoids more invasive surgery or radiation in many cases, making it a preferred option for early laryngeal cancer.
Before: Trans Oral Laser Cordectomy for Cancer
After: Trans Oral Laser Cordectomy for Cancer
This combined procedure treats laryngeal stenosis, a narrowing of the airway that can cause breathing and voice problems. The CO2 laser is used to carefully remove scar tissue or abnormal growths, and dilation stretches the airway open to restore normal airflow.
Surgery is done under general anesthesia using a microscope and laser equipment. Balloon or rigid dilators may be used to expand the narrowed area. Postoperative care often includes voice rest, steroid or anti-inflammatory medications, and sometimes repeat procedures. Risks include recurrence of the stenosis, temporary voice changes, and airway irritation. This approach helps improve breathing while preserving voice as much as possible.
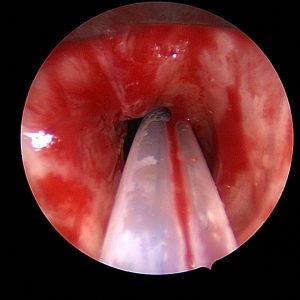
Before: CO2 Laser Excision for Stenosis
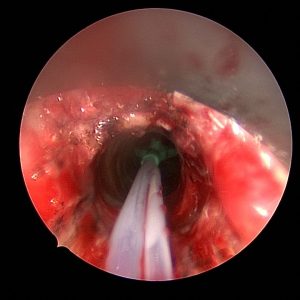
After: CO2 Laser Excision for Stenosis
This procedure improves vocal cord function in patients with vocal cord atrophy, scarring, or paralysis. Fat is harvested from another part of the patient's body—often the abdomen or thigh—and carefully injected into the vocal cord to restore bulk and improve closure during speech. This fat injection helps improve voice strength and reduce breathiness.
The procedure is done under general anesthesia using an operating microscope. A small incision is made to harvest fat, which is then purified and injected precisely into the vocal fold. Recovery typically includes voice rest for several days, and voice therapy is often recommended afterward to help optimize vocal performance. Some of the injected fat may be absorbed over time, so occasional touch-up procedures may be needed. Most patients experience a noticeable improvement in vocal strength and endurance.
VoiceGel is a biocompatible, temporary filler injected into the vocal fold to improve vocal cord closure. It's commonly used for temporary vocal fold paralysis, vocal cord weakness, or diagnostic purposes to assess if a more permanent injection will benefit. The gel provides immediate voice improvement and naturally resorbs over a few months.
During this procedure, which is performed under general anesthesia, the surgeon uses a micro laryngoscope to view the vocal folds and inject the material with precision. Patients typically notice an improvement in voice quality soon after the procedure. Since it is temporary, the effects wear off over time, making this a good option for short-term correction or trial before a permanent solution. Recovery involves limited voice use and close follow-up to assess results.
Cidofovir is an antiviral medication used to treat recurrent respiratory papillomatosis (RRP), a condition in which benign HPV-related growths develop in the airway. During this procedure, after removing the papillomas (often with a laser), the surgeon injects Cidofovir directly into the affected area to help reduce the recurrence of the disease.
The injection is done during microlaryngoscopy under general anesthesia. It is often part of a long-term management plan for patients who experience frequent recurrences of papillomas. Recovery is similar to other microlaryngoscopy procedures involving voice rest and follow-up endoscopic evaluations. While Cidofovir is not a cure, it can decrease many patients' severity and frequency of outbreaks.
Steroid injections are used to reduce inflammation, scarring, or swelling in the vocal folds. They are commonly given to patients with chronic laryngitis, vocal fold nodules, granulomas, or after vocal fold surgery to help promote healing and reduce scar tissue formation.
The steroid is injected directly into the vocal fold tissue. The medication helps calm inflammation and support smoother, more flexible vocal cord movement. Patients typically follow up with voice rest and therapy. This low-risk approach is often used to enhance recovery from other vocal cord surgeries or treat specific voice-related inflammatory conditions.
This procedure treats vocal cord scarring, thinning, or atrophy that affects voice quality. PRP (Platelet-Rich Plasma) and fat are both natural substances derived from the patient's own body. Fat can help restore lost volume and cushion the vocal folds, while PRP, which is rich in growth factors, supports tissue healing and regeneration. When used together, they can improve vocal fold pliability and vibratory function, leading to a stronger, clearer voice.
The procedure is done under general anesthesia using a surgical microscope. A small incision is made in the vocal fold surface, and fat (usually harvested from the abdomen or thigh) and/or PRP are injected into the vocal fold muscle. Recovery typically involves voice rest for several days to allow the tissues to settle and heal. Most patients gradually resume speaking, and the voice often improves over several weeks. Follow-up may include voice therapy to optimize the results. Because fat may be reabsorbed over time, some patients may need a second procedure later.
This procedure is most commonly used to treat spasmodic dysphonia, a voice disorder in which the vocal cords involuntarily spasm during speech. Botox (botulinum toxin) is a well-established treatment that temporarily weakens the overactive muscles, allowing for smoother, more controlled speech. Botox may also be used in select cases of vocal tremor or other laryngeal dystonias.
When performed under general anesthesia with a laryngoscope and surgical microscope, this procedure allows for precise placement of Botox into the vocal muscles. It is generally very safe and takes only a few minutes. Afterward, patients may experience temporary breathiness, reduced vocal strength, or mild swallowing difficulty, which usually resolves within a few days to weeks as the muscles adjust. The full benefit typically appears within a week and lasts around 3–6 months. Repeat injections are often needed to maintain voice improvement.
Microlaryngoscopy with Botox injection for Abelchia (inability to burp) is a specialized surgical procedure to help patients who are unable to belch due to tightness or dysfunction of the cricopharyngeus muscle,a component of the upper esophageal sphincter. Under general anesthesia, a rigid laryngoscope is used to access the upper airway, and a small amount of botulinum toxin is precisely injected into the cricopharyngeus muscle. This weakens the muscle just enough to allow trapped air to be released, relieving symptoms such as bloating, gurgling, chest pressure, and abdominal discomfort. The procedure is performed on an outpatient basis, and most patients go home the same day. Recovery is generally quick, and patients can return to a normal diet as tolerated. Many people begin to burp within a few days to a week, with symptom relief often continuing for several months or longer.
The following video is a patient one week after Botox injection. She complains of some swallow dysfunction but is happy she can belch again.
KTP (potassium titanyl phosphate) laser ablation treats vascular lesions, papillomas (caused by HPV), or certain benign and malignant vocal fold growths. The KTP laser is unique because it targets blood vessels, allowing for precise treatment of lesions with minimal damage to the surrounding tissue — making it an excellent tool for preserving vocal quality.
During the procedure, the patient is placed under general anesthesia, and a laryngoscope is used to expose the vocal folds. The surgeon then uses the KTP laser, delivered through a thin fiber, to gently shrink or remove the lesion. Because it causes less thermal damage than other lasers, healing is typically quicker, and voice outcomes are often excellent. Patients usually need voice rest for a few days afterward, followed by a gradual return to speaking. In some cases, especially with papillomas, multiple treatments may be necessary. Follow-up may include repeat scopes and voice therapy.
This advanced procedure repairs areas of damaged or missing vocal fold tissue. It is often performed in cases where previous surgery, trauma, or disease has caused scarring or tissue loss, leading to a stiff, breathy, or hoarse voice. The goal is to restore the smooth mucosal surface of the vocal fold to vibrate properly for sound production.
Under general anesthesia, the surgeon uses a microscope and delicate instruments to remove scarred or damaged areas. A small graft — often taken from the patient’s own mouth lining (buccal mucosa) — is then precisely placed over the area to replace the lost tissue. After surgery, patients are usually asked to rest their voice for at least a week. Recovery also involves follow-up with laryngoscopy to check healing, and often voice therapy to retrain the voice. Results can be excellent but may take time to fully develop.
This procedure improves vocal quality by adjusting the position or tension of the vocal folds. It is typically used to treat vocal fold paralysis, weakness, or asymmetry that causes a breathy or weak voice. During microlaryngoscopy, laryngoplasty techniques are performed internally — often by injecting material or reshaping vocal structures to improve closure and voice production.
Performed under general anesthesia, the vocal folds are accessed through the mouth using a surgical microscope. The surgeon may inject fat, filler or use sutures or implants to reposition the folds. The results can lead to better vocal strength, clarity, and endurance. Most patients recover quickly, with some voice rest required. The voice often improves within days, but optimal results are usually seen over several weeks. Risks are minimal, and follow-up includes voice therapy to help the patient adapt to the new vocal mechanics.
This combined procedure treats Zenker’s diverticulum, a pouch that forms in the upper esophagus and traps food. This can lead to difficulty swallowing, coughing, and even aspiration (food entering the airway). The surgery also involves cutting the cricopharyngeal muscle, which can become overly tight and contribute to the problem.
Performed under general anesthesia, the surgeon accesses the pouch through the mouth or neck and divides the wall between the esophagus and the pouch (diverticulotomy), allowing food to flow normally. At the same time, the tight muscle at the upper esophagus is cut (myotomy) to reduce pressure and prevent recurrence. Most patients notice improvement in swallowing. Recovery involves a short hospital stay, starting with a liquid diet that gradually advances. Risks include bleeding, infection, or temporary hoarseness, but complications are uncommon in experienced hands.
Tubed supraglottoplasty is a procedure to treat laryngomalacia and aspiration, a condition where soft tissues above the vocal cords collapse inward during breathing, causing noisy breathing or airway obstruction — most common in infants and young children. This surgery reshapes or stiffens those tissues to improve airflow. When done for aspiration, the height of the larynx is changed to prevent spillover of food and liquids into the larynx.
During the procedure, which is done under general anesthesia, a laryngoscope is used to access the upper larynx. The surgeon carefully trims or repositions floppy tissue, often creating a differently shaped airway. Sometimes, tiny tubes (stents) are temporarily placed to hold the tissues in their new position as they heal. Recovery depends on the age and condition of the patient, but many experience immediate improvement in breathing and feeding. Postoperative care includes close monitoring for airway swelling and follow-up laryngoscopy. In most cases, voice and swallowing are unaffected or improve as breathing normalizes.
This procedure involves harvesting a small section of the inner cheek lining (buccal mucosa) as a graft to repair or reconstruct parts of the airway or vocal cords. It's often used when significant tissue loss, scarring, or stenosis (narrowing) in the throat or larynx cannot be repaired with local tissue alone.
Under general anesthesia, a graft is removed from the inside of the cheek — an area that heals quickly — and is then shaped and sutured into the affected area. The goal is to restore normal structure and function while minimizing voice or airway compromise. Recovery involves voice rest, wound care, and sometimes temporary stents or breathing support, depending on the location of the graft. Voice therapy and follow-up scopes are essential to guide healing. The donor site in the mouth may feel sore for a few days but generally heals without long-term issues.
A split-thickness skin graft involves taking a thin layer of skin from one part of the body (usually the thigh) and using it to reconstruct another area that has lost skin or tissue. In laryngology, it may be used to cover large mucosal defects in the throat, trachea, or neck following tumor removal or trauma.
The surgery is performed under general anesthesia. The graft is harvested, placed over the defect, and then secured with fine sutures or tissue glue. A dressing or stent may be used to protect the area during healing. Recovery can vary depending on the size and location of the graft, but patients may need voice rest, antibiotics, and regular monitoring to ensure graft success. The donor site typically heals in 1–2 weeks and may feel like a scrape or mild burn. Graft survival is usually excellent when kept moist and undisturbed.
Laryngeal stenting keeps the airway open after surgery or injury, especially in patients with laryngeal collapse, scarring, or after reconstructive procedures. A stent — typically made of silicone — is placed inside the larynx to maintain space and support healing tissues.
This procedure is done under general anesthesia and is often part of a larger reconstructive surgery. Depending on the treated condition, the stent remains in place for several days to weeks. Patients may have limited voice use or require alternative communication methods during this time. They are closely monitored for stent displacement, irritation, or infection. Once healing is sufficient, the stent is removed in a follow-up procedure. Voice and airway function are then reassessed, and additional therapies like voice training or minor revision surgery may be needed.
Foreign body removal is an emergency or urgent procedure to extract objects accidentally inhaled or swallowed. Children are most often affected, but adults can also aspirate or ingest items such as food, bones, dental appliances, or small objects. Depending on where the item is lodged — the larynx (voice box), trachea (windpipe), or esophagus (swallowing tube) — symptoms may include coughing, choking, wheezing, pain, or inability to swallow or speak.
The procedure is done under general anesthesia using a rigid or flexible scope and grasping tools. The surgeon carefully removes the object while minimizing trauma to the delicate airway and surrounding tissues. Most patients recover quickly and resume normal activities shortly after. Rare complications include bleeding, swelling, or vocal changes, especially if the object was sharp or in place for a long time. Follow-up depends on the situation but may involve imaging or repeat endoscopy to ensure no remaining injury.
This procedure opens narrowed airways (a condition called stenosis) and removes abnormal tissue that may be blocking airflow. It's commonly performed in patients with scar tissue, tumors, or inflammation in the trachea or bronchi. The goal is to restore normal breathing, reduce symptoms like wheezing or shortness of breath, and prevent airway collapse.
The procedure is done under general anesthesia. A bronchoscope — a thin, flexible, or rigid tube with a camera — is inserted through the mouth or nose into the windpipe. If there is a narrowing, a balloon or mechanical dilator is used to widen the airway. Any obstructive tissue is then carefully removed with surgical instruments or a laser. Afterward, the patient is monitored for swelling or breathing difficulty. Recovery is generally quick, though voice and breathing may differ for a few days. Some patients with chronic narrowing may need repeat procedures or follow-up imaging to maintain results.
This procedure combines diagnosis and treatment for conditions affecting the esophagus — such as trouble swallowing (dysphagia), muscle spasms, strictures, or suspected growths. Using a long, flexible scope, the doctor inspects the inside of the esophagus, collects tissue samples if needed (biopsy), injects Botox to relax tight muscles, and stretches narrowed sections (dilation) to improve swallowing.
The procedure is typically done under general anesthesia. A small camera is passed through the mouth and down the throat. Biopsies may be taken for testing. Botox is injected into areas where the esophagus is overly tight, often helping ease spasms or achalasia. Dilation is performed using inflatable balloons or soft dilators. Patients may have a sore throat afterward and must avoid eating or drinking for a few hours. Botox effects develop over a few days and can last several months. Follow-up depends on the underlying condition, but most patients experience a noticeable improvement in swallowing comfort.
Open laryngeal surgery refers to any surgical procedure in which the larynx (voice box) is accessed through an incision in the neck rather than through the mouth. These surgeries are performed when minimally invasive (endoscopic) techniques are not enough—for example when removing large tumors, repairing severe injuries, or reconstructing damaged structures of the larynx.
Phonosurgery is a set of specialized surgical procedures to improve or restore the voice by modifying the vocal folds. The different types (I–IV) refer to Isshiki's classification system, which describes how the vocal fold is repositioned or reshaped:
Type I (Medialization): Moves a paralyzed or weak vocal fold toward the midline to help it close during speech.
Type II (Lateralization): Used to treat spasmodic dysphonia by moving the vocal fold slightly outward to reduce tension.
Type III (Relaxation): Shortens the vocal fold to lower pitch, often used in transgender voice surgery or certain hyperfunctional voice disorders.
Type IV (Tensioning): This technique lengthens the vocal fold to raise pitch. It is sometimes used to feminize the voice or strengthen weak vocal folds.
These procedures are typically performed under sedation anesthesia, though some can be done under local anesthesia with the patient awake (to fine-tune voice outcome). Recovery includes voice rest for several days, followed by voice therapy to train the new vocal dynamics. Most patients notice a gradual improvement over weeks. Risks include hoarseness, over- or under-correction, or need for revision surgery, but outcomes are generally excellent when tailored to the individual's voice goals.
Laryngofissure is a rare and specialized open surgical procedure used when the larynx must be opened through the front (midline) to access deep or complex problems. It may be used to remove large benign or malignant tumors, correct congenital anomalies, or treat significant trauma. This approach gives the surgeon a direct view and full access to the vocal cords and supporting structures.
Under general anesthesia, a vertical incision is made in the front of the neck, and the thyroid cartilage is split apart to open the larynx. After addressing the underlying issue — such as tumor removal or reconstruction — the larynx is carefully closed and often stabilized with sutures or a stent. Recovery involves a hospital stay, possible temporary tracheostomy, and strict voice rest. The voice may change after surgery depending on the area treated. Risks include infection, scarring, vocal changes, or airway complications, and patients are monitored closely with follow-up scopes and speech therapy as needed.
This procedure is performed to treat a fracture of the larynx — typically the result of blunt trauma to the neck (e.g., car accidents, sports injuries, or assault). Prompt repair is crucial to restore the airway, preserve the voice, and prevent long-term breathing or swallowing issues.
During the operation, the surgeon makes an incision in the neck to access the damaged larynx. The broken cartilage or bone is realigned and secured, and torn soft tissues or vocal folds are repaired. Depending on the severity, a temporary tracheostomy may be placed to protect the airway during healing. Recovery includes hospitalization, voice rest, and gradual return to normal activities. Most patients require follow-up imaging and voice therapy. Many regain normal or near-normal voice and breathing if treated early and correctly. Risks include hoarseness, vocal fold stiffness, airway narrowing, or needing revision surgery.
These are organ-preserving surgeries designed to treat laryngeal cancer while maintaining as much voice and swallowing function as possible. Rather than removing the entire voice box (as in total laryngectomy), these surgeries remove only the cancerous portion of the larynx.
Partial laryngectomy refers broadly to removing part of the larynx.
Hemilaryngectomy involves removing one side of the larynx, often including one vocal fold.
Supraglottic laryngectomy removes structures above the vocal folds (like the epiglottis), preserving the voice.
CHP (Cricohyoidopexy) and CHEP (Cricohyoidoepiglottopexy) are advanced variations used to preserve swallowing while removing cancer-bearing areas.
These surgeries are performed through a neck incision under general anesthesia. A temporary tracheostomy is often required during healing. Recovery involves a hospital stay, speech and swallowing therapy, and close follow-up with scopes. The voice will change depending on the amount of tissue removed — some hoarseness or breathiness is expected. Swallowing usually improves over time. Risks include aspiration (food going down the wrong way), need for feeding tube support, or recurrence of cancer.
These procedures are used to treat bilateral vocal fold paralysis, where both vocal cords are stuck in a closed position, blocking the airway. An arytenoidectomy involves removing part of one of the arytenoid cartilages (which control vocal fold movement) to open the airway. An arytenoidpexy involves repositioning and securing the arytenoid cartilage to improve breathing while trying to preserve voice and swallowing.
The surgery is performed under general anesthesia through a neck incision or sometimes endoscopically, these procedures help patients breathe more freely without relying on a permanent tracheostomy. When done for voice, it repositions the arytenoid cartilage into the proper position. There is a brief hospital stay after surgery to monitor breathing and swallowing. Recovery includes voice rest, monitoring for airway swelling, and gradual reintroduction of speech. The voice may become weaker or breathier after the procedure due to the more open vocal folds, but most patients can communicate effectively. Risks include scarring, aspiration, or need for revision surgery, but results are often life-changing for those struggling to breathe.
This complex reconstructive procedure expands a narrowed or collapsed airway, often due to congenital problems, trauma, or prolonged intubation. A rib graft (usually harvested from the patient) is shaped and used to widen the airway, and a stent is placed to hold the airway open during healing.
Under general anesthesia, the neck is opened to access the airway. The narrowed area is split or removed, and the rib graft is placed to provide structural support. A stent is inserted and remains for several weeks. Patients are monitored closely during hospitalization for signs of swelling or infection. After the stent is removed, breathing and voice are reassessed. Recovery involves frequent follow-ups, and the voice may initially be hoarse or weak but often improves with therapy. This surgery is highly specialized and performed only by surgeons experienced in airway reconstruction.
Tracheal resection is a procedure used to treat narrowing (stenosis) or tumors in the trachea (windpipe). The narrowed or diseased segment of the trachea is removed, and the two healthy ends are reconnected. This surgery restores normal airflow and can be curative in both benign and cancerous conditions.
The procedure is done under general anesthesia through a neck or chest incision. A breathing tube is placed below the area to be removed. Once the diseased portion is excised, the trachea is sutured back together. Recovery includes a hospital stay, close airway monitoring, and limited neck movement to protect the healing site. Most patients breathe more easily right away. Voice is usually unaffected unless the narrowing is near the vocal cords. Risks include wound separation, infection, or scar tissue regrowth. Long-term success is excellent with proper follow-up and sometimes includes additional procedures like dilation.
A tracheal trough procedure is a surgical technique used to create a larger or more stable airway opening in the trachea. It may be performed as part of complex airway reconstruction, often when there has been long-standing tracheostomy use, subglottic stenosis, or tracheomalacia (weak or collapsing trachea). The goal is to improve breathing without the need for ongoing airway tubes.
In this procedure, the surgeon reshapes or removes part of the front of the trachea and may use grafts or stents to maintain the new, wider contour. It is done under general anesthesia, and recovery depends on the extent of the reconstruction. Some patients may need a temporary stent or tracheostomy during healing. Postoperative care includes frequent endoscopic evaluations, airway humidification, and voice rest if vocal structures are involved. This procedure is highly individualized and planned according to airway imaging and scope findings.
This complex surgery treats the combined narrowing of the larynx and trachea, often due to scarring from intubation, autoimmune disease, or trauma. It involves removing and reconstructing the affected airway segment using nearby tissue, grafts, or cartilage support. The goal is to restore both breathing and voice function as fully as possible.
The procedure is done under general anesthesia through a neck incision. The narrowed airway is resected, and the remaining larynx and trachea are joined. Depending on the severity of the case, stents or grafts may be used, and a temporary tracheostomy is often placed. Recovery includes hospitalization, strict airway precautions, and regular endoscopic follow-up. Patients may notice voice changes depending on how close the repair was to the vocal folds. Risks include scarring, recurrence of stenosis, or difficulty swallowing, but many patients experience excellent improvement in breathing and function with proper post-op care.
Zenker’s diverticulectomy is a surgical procedure to remove a pouch-like pocket (diverticulum) that can form at the back of the throat, just above the esophagus. This pouch traps food and liquids, leading to symptoms like bad breath, coughing after eating, choking, and difficulty swallowing.
The surgery can be done through the mouth (endoscopic approach) or through an incision in the neck (open approach), depending on the size and location of the diverticulum. In both cases, the pouch is removed or opened into the esophagus, and the tight muscle (cricopharyngeus) contributing to the problem is cut. Recovery typically includes a short hospital stay, a liquid diet at first, and a gradual return to solid foods. Voice and breathing are usually unaffected, and swallowing improves significantly. Risks include infection, bleeding, or leak at the surgical site, though complications are uncommon with experienced surgeons.
Cricopharyngeal myotomy is a targeted surgical procedure to treat dysphagia (difficulty swallowing) caused by a tight or dysfunctional cricopharyngeus muscle at the top of the esophagus. This muscle should relax during swallowing, but in some people, it stays tight, leading to a feeling of food getting stuck, coughing, or regurgitation.
Under general anesthesia, the muscle is carefully cut, either through a small neck incision or endoscopically through the mouth. Surgical myotomy allows the upper esophagus to open more easily during swallowing. Most patients can eat more comfortably within a few days. A liquid or soft diet is usually recommended during the initial recovery phase. Risks include temporary throat soreness, aspiration, or scarring, but the procedure has a high success rate and significantly improves the quality of life for many patients.
Hypopharyngeal pharyngoplasty is a reconstructive surgery used to reshape or repair the lower part of the throat (hypopharynx), especially after tumor removal, trauma, or congenital deformities. It may also be performed to reduce airway collapse in severe obstructive sleep apnea when other treatments have failed.
The surgeon repositions and reinforces tissues using sutures, flaps, or grafts during the procedure. Pharyngoplasty is aimed at restoring swallowing and speech function. General anesthesia is required, and recovery includes a hospital stay, possible feeding tube support, and speech or swallowing therapy. Healing time varies depending on the complexity, but the goal is always to preserve or regain essential functions like breathing, eating, and speaking. Risks include scarring, aspiration, or wound breakdown, but outcomes are often favorable with good post-op care.
Palatoplasty is a surgical procedure to reconstruct or repair the soft palate. It is usually performed on children with cleft palates, but it can also be used on adults with velopharyngeal insufficiency (VPI)—a condition in which the soft palate doesn't close properly during speech, causing a nasal-sounding voice or air leakage.
The surgery involves repositioning and suturing the soft palate muscles to improve closure during speaking and swallowing. It's done under general anesthesia, and recovery usually involves a soft diet, pain management, and speech therapy. Children often begin to speak more clearly within weeks, though long-term therapy may be needed. In adults, it may improve speech quality and reduce nasal regurgitation of food. Risks include wound breakdown, fistula formation, or the need for additional surgeries, but most patients experience clear functional gains.
Tonsillectomy is a surgical procedure to remove the tonsils, which are small glands located at the back of the throat. It is commonly performed in children or adults who experience repeated throat infections (tonsillitis), large tonsils causing sleep or breathing problems, chronic tonsil stones, or bad breath. In some cases, a tonsillectomy may also be done if there is concern about abnormal or potentially cancerous tissue.
The procedure is done under general anesthesia and usually takes less than an hour. The tonsils are removed through the mouth using specialized tools, with no external cuts. Recovery typically takes 7 to 10 days and involves a sore throat, difficulty swallowing, and fatigue. Pain medication and a soft or cold diet (like popsicles or ice cream) are recommended. The most important thing is to stay well hydrated. There is a small risk of bleeding in the days after surgery, so any fresh blood should be reported to your doctor immediately. Most people feel much better after they've healed and often notice improved breathing or fewer infections.
An adenoidectomy removes the adenoids, a mass of tissue behind the nose and throat. Adenoids can become enlarged due to frequent infections or allergies and may cause snoring, nasal obstruction, mouth breathing, or chronic ear infections. This procedure is often performed in children, sometimes alongside tonsillectomy.
Adenoidectomy is done under general anesthesia and is performed through the mouth, so there are no external incisions. It is a short and safe procedure, often done as outpatient surgery. Most children recover quickly, with only mild sore throat or nasal congestion for a few days. Breathing through the nose typically improves, and snoring often decreases. Risks are low but can include bleeding, infection, or a temporary nasal-sounding voice as the throat adjusts. Follow-up is usually straightforward; most adults and children return to school or work within a few days.
Septoplasty is surgery to straighten the nasal septum—the thin wall of cartilage and bone that divides the two sides of the nose. If the septum is deviated or crooked, it can block airflow and cause nasal congestion, snoring, nosebleeds, or recurrent sinus infections. Septoplasty is not a cosmetic procedure; it’s focused on improving breathing.
The procedure is performed under general or local anesthesia. The surgeon repositions or removes parts of the deviated septum to open the nasal passages through a small incision inside the nose. There are no external scars. Some patients may have soft internal splints for a few days to support healing. Recovery usually includes mild nasal stuffiness, pressure, or drainage for about a week. Avoiding heavy activity and blowing the nose is essential during healing. The procedure is highly effective, and many patients notice significantly improved breathing once the swelling subsides.
Turbinate resection (or reduction) is a procedure to shrink or remove part of the turbinates — structures inside the nose that warm, humidify, and filter the air we breathe. When these become chronically enlarged due to allergies, infection, or anatomical issues, they can block airflow and contribute to congestion, mouth breathing, or snoring.
The surgery is often done alongside septoplasty and can be performed under general or local anesthesia. The turbinates are reduced using various methods (trimming, radiofrequency, or cautery), all done through the nostrils with no external incisions. Recovery is usually mild, with some congestion and nasal drainage for several days. Saline sprays and avoiding nose-blowing help with healing. Most patients breathe more easily and feel less congested after recovery. Complications are rare but can include dryness or crusting in the nose.
A nasal polypectomy is a procedure to remove nasal polyps — soft, non-cancerous growths that form in the lining of the nose or sinuses, often due to chronic inflammation, allergies, or sinus infections. These polyps can cause nasal blockage, reduced sense of smell, postnasal drip, or recurrent sinus infections.
The procedure is done endoscopically through the nostrils under general or local anesthesia. The polyps are carefully removed without cutting through the skin. Recovery usually involves mild discomfort, nasal congestion, or drainage for a few days. Saline sprays or steroid rinses are often recommended to promote healing and reduce recurrence. Follow-up may include allergy treatment or long-term nasal steroid use. While polyps can regrow, many patients experience significant improvement in nasal breathing and sinus symptoms.
Endoscopic sinus surgery is used to open blocked sinus passages and improve drainage. It’s commonly performed for chronic sinusitis that doesn’t improve with medication, nasal polyps, or structural problems like narrow sinus openings. The goal is to reduce infection, improve airflow, and restore normal sinus function.
The procedure is done under general anesthesia using an endoscope — a small camera inserted through the nostrils. The surgeon removes obstructions, widens sinus openings, and may clear out infected tissue. No external incisions are made. Recovery includes nasal congestion, mild bleeding, and the need for saline rinses to keep the sinuses clean. Most patients can return to normal activities within a week. Continued care with nasal sprays or allergy management is needed. This minimally invasive surgery has a high success rate and can significantly improve breathing, sense of smell, and quality of life.
A lymph node biopsy is a procedure to remove a small portion or all of a lymph node for testing. It's done when a node feels abnormally large, hard, or tender or when imaging suggests changes that could indicate infection, inflammation, or cancer. Lymph node biopsy helps determine the cause of the swelling and guides further treatment.
The biopsy is usually performed under local or general anesthesia, depending on the location and size of the lymph node. A small incision is made near the node — commonly in the neck — and the tissue is removed and sent to a lab. Recovery is quick, with minimal discomfort and a small scar. Most patients resume normal activities within a day or two. Results typically come back within a week. Risks are low but can include bleeding, infection, or nerve irritation, depending on the node's location.
This procedure involves the complete removal of one or more lymph nodes, usually as part of cancer diagnosis or treatment. Unlike a biopsy, which takes a sample, this surgery is done when the node is known or suspected to contain disease (like metastatic cancer or lymphoma) or if it's persistently enlarged or causing problems.
Performed under general anesthesia, the surgeon makes an incision near the affected area (usually in the neck or under the jaw), identifies the lymph node, and carefully removes it. The incision is then closed with sutures. Recovery involves some swelling and discomfort, but patients are usually able to go home the same day. Depending on the location, the area may have temporary numbness or stiffness. A pathologist examines the removed node to guide future care. Risks are generally low but can include infection, nerve injury, or fluid buildup (seroma).
This procedure removes the submandibular (or submaxillary) salivary gland, located beneath the lower jaw. It may be performed if there are chronic infections, stones blocking the duct, or tumors (most of which are benign but occasionally malignant).
The surgery is done under general anesthesia through an incision under the jawline. The gland is carefully removed while protecting nearby nerves that control tongue movement and feeling. A drain may be placed temporarily to prevent fluid buildup. Recovery includes a few days of swelling, mild pain, and possible temporary numbness under the chin or tongue. Most people return to normal activities within a week. Follow-up includes monitoring the incision and reviewing pathology if a tumor is involved. Long-term issues are rare, and most patients experience relief from their symptoms.
This is a minor surgical procedure used to treat an abscess, a collection of pus caused by infection. Abscesses in the head and neck area—such as in the skin, lymph nodes, or salivary glands—can cause pain, swelling, redness, and fever if not treated promptly.
The skin is cleaned under local anesthesia (or general, if the abscess is deep or in a sensitive area), and a small incision is made to allow the pus to drain. The area may be irrigated and packed with gauze. Antibiotics are usually prescribed afterward. Patients typically feel relief almost immediately, and the area heals over several days. Follow-up may be needed to ensure full resolution. Risks are minimal but can include scarring or recurrence if the underlying infection isn't fully treated.
Also known as peritonsillar abscess drainage, this procedure treats a collection of pus that forms near the tonsil — a painful and sometimes serious complication of tonsillitis. Symptoms include severe sore throat (usually one-sided), difficulty swallowing, fever, swollen lymph nodes, and muffled voice.
Drainage is typically performed under local anesthesia, although sedation may be used for comfort. A small incision is made near the abscess to release the pus. In some cases, a needle may be used instead. Antibiotics are given, and pain improves quickly once the abscess is drained. Recovery includes hydration, rest, and soft foods. Rarely, if abscesses recur or are severe, a tonsillectomy may be recommended later. Risks include bleeding or recurrence, but this procedure is generally safe and effective.